

A jaw that clicks upon waking, a dull pain in front of the ear, unexplained headaches: temporomandibular joint (TMJ) disorders often go unnoticed for months. Yet they are common, particularly among women between 20 and 40 years old, and most progress favorably when diagnosed early.
I am Dr. Daniil Klimovich, an orthodontist at the DentalGeneva clinic. I manage TMJ disorders as part of a multidisciplinary approach, alongside physiotherapists and maxillofacial surgeons. In this article, I explain how to recognize these disorders, what causes them, and the treatments available in Geneva, from the simplest to the most specialized.
Key Takeaways
The temporomandibular joint (TMJ) is the joint that connects the lower jaw to the skull, just in front of each ear. A TMJ disorder, or temporomandibular dysfunction, encompasses all pain and dysfunction of this joint and the muscles that control it. The most common signs are jaw pain, clicking, locking, headaches, and teeth clenching. The majority of cases are treated without surgery, provided an accurate diagnosis is made first.
In this article
- What is the TMJ?
- Symptoms: When to consult?
- TMJ disorders we treat
- Our diagnostic approach
- Our TMJ treatments
- Are you a practitioner? Refer a patient
- Frequently asked questions
What is the TMJ?
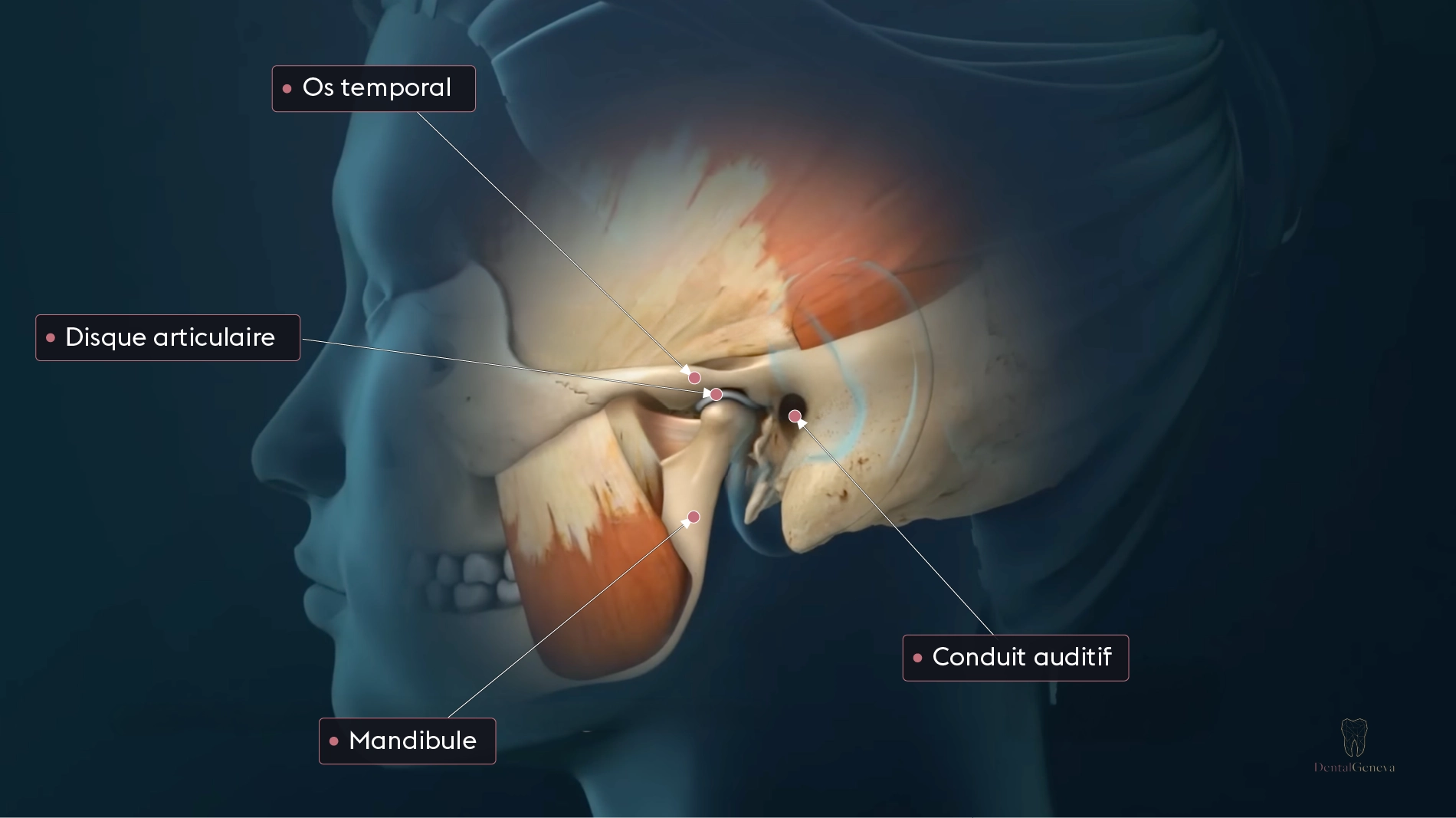
The TMJ is one of the most frequently used joints in the body. You use it every time you eat, speak, or yawn—several hundred times a day. Located on either side of the face, it connects the jaw condyle to the temporal bone of the skull.
Between the two bony surfaces lies a small disc of cartilage, the articular disc, which cushions movements and allows the jaw to glide smoothly. Around the joint, several masticatory muscles handle opening, closing, and lateral movements. A disorder can involve the disc, the joint itself, the muscles, or several of these elements simultaneously.
These disorders are common. A recent systematic review estimates the global prevalence of TMJ disorders at nearly 30%. This figure includes mild forms; painful forms requiring treatment are less frequent, ranging from 5% to 12%. These disorders affect women two to four times more often than men, peaking between ages 20 and 40. Hormonal variations and certain characteristics of joint tissues are among the hypotheses proposed to explain this difference.
They are also often misidentified. TMJ pain can radiate to the ear, temple, or cheek, and may be confused with an ear infection, migraine, or sinusitis. Many patients first consult for these reasons before the joint origin is recognized.
Symptoms: When to consult?
TMJ disorders manifest through various signs, which may appear alone or in combination:
- Jaw or facial pain, sometimes in front of the ear
- Clicking or popping sounds when opening and closing
- Jaw that locks or no longer opens normally
- Recurrent headaches, especially upon waking
- Tinnitus or a sensation of a clogged ear
- Neck and shoulder pain
- Bruxism, i.e., teeth clenching or grinding
An isolated and temporary sign is generally nothing to worry about. However, if several of these signs have affected you for more than a few weeks, or if the pain interferes with chewing and sleep, a TMJ evaluation is warranted. An early diagnosis often prevents mild discomfort from becoming chronic pain.
TMJ Evaluation
Persistent jaw discomfort deserves an examination
An assessment helps identify the origin of the disorder and prevents it from becoming permanent.
Book an appointment →TMJ disorders we treat
The term temporomandibular dysfunction covers several distinct clinical situations. Differentiating them is essential, as the management approach varies.
Disc displacement with reduction
The articular disc slides out of position and then returns to place during movement. This return produces the characteristic click when opening the mouth. This situation is usually benign but warrants monitoring to prevent it from progressing.
Disc displacement without reduction
The disc remains stuck forward and no longer returns to its place. Mouth opening becomes limited, often painful, and the click disappears. This form requires prompt management to preserve joint mobility.
Capsulitis and arthralgia
This is an inflammation of the joint and its envelope, the capsule. The pain is localized, often triggered by pressure or chewing.
Muscle pain
The masticatory muscles contract excessively and develop trigger points. These myalgias are frequently linked to stress and bruxism. They can explain the pain on their own, even when the joint is healthy.
TMJ Osteoarthritis
Osteoarthritis corresponds to progressive wear of the joint surfaces. It results in crepitus, stiffness, and sometimes visible changes on imaging. It more often affects mature patients.
Bruxism
Bruxism is the involuntary clenching or grinding of teeth. A distinction is made between sleep bruxism and awake bruxism. It places heavy strain on the TMJ and muscles and can be associated with stress as well as nocturnal respiratory disorders such as snoring and sleep apnea.
| Disorder | Characteristic sign | Management approach |
|---|---|---|
| Disc displacement with reduction | Click upon opening, disc returns to place | Monitoring, splint |
| Disc displacement without reduction | Limited opening, no click | Prompt management |
| Capsulitis and arthralgia | Localized joint pain | Anti-inflammatories, splint |
| Muscle pain | Tense muscles, trigger points | Physiotherapy, stress management |
| TMJ Osteoarthritis | Crepitus, wear on imaging | Injections, follow-up |
| Bruxism | Teeth clenching or grinding | Splint, stress management |
Our diagnostic approach
The same symptom can correspond to several distinct disorders. This is why we never treat blindly: we first establish an accurate diagnosis.
The consultation begins with a detailed interview, the anamnesis, which traces the history of the pain, clenching habits, stress, and sleep quality. This is followed by a complete clinical examination: measuring mouth opening, palpating muscles and the joint, and listening for joint sounds.
When necessary, we supplement this with appropriate imaging: panoramic X-ray, cone beam computed tomography (CBCT), or magnetic resonance imaging (MRI) to visualize the disc and soft tissues. Finally, we analyze the occlusion—the way the teeth fit together—as dental malocclusion can contribute to the disorder.

Our TMJ treatments
Management ranges from the simplest devices to the most specialized procedures. In the vast majority of cases, conservative treatments are sufficient.
The Michigan splint
The Michigan splint is a flat splint worn on the upper arch. It decompresses the joint and relaxes the masticatory muscles. It is the first-line treatment and the most widely used orthosis in the world for TMJ disorders. A meta-analysis confirms its effect on pain reduction in the short term, as well as an improvement in mouth opening.

Mandibular repositioning splint
In some cases, such as disc displacement with reduction, a splint that slightly advances the jaw can relieve the joint. This device is similar in principle to a mandibular advancement device (MAD) used for snoring, but its adjustment and objective are different. In a patient with both a TMJ disorder and snoring, coordinated management can sometimes address both problems. A sleep apnea risk assessment test helps guide this decision.
Maxillofacial physiotherapy
Muscle disorders respond well to rehabilitation. In collaboration with physiotherapists specializing in maxillofacial rehabilitation, the treatment combines exercises, manual therapy, ultrasound, and electrical stimulation (TENS). This approach often complements the use of a splint.
Injections
When pain resists conventional treatments, or in cases of osteoarthritis, injections may be proposed in collaboration with a maxillofacial surgeon. Platelet-rich plasma (PRP) injections use growth factors from the patient’s own blood. Available data show a reduction in pain for TMJ osteoarthritis, with a level of evidence that is still limited. Other injections, based on hyaluronic acid or corticosteroids, are also possible depending on the indication.
Surgical options
Resorting to surgery remains rare and only occurs after the failure of conservative treatments. It ranges from minimally invasive procedures, such as arthrocentesis or arthroscopy, to more extensive interventions in complex cases. We work in a network with maxillofacial surgeons for these situations.
Are you a practitioner? Refer a patient
This section is for dentists, orthodontists, physiotherapists, osteopaths, doctors, ENTs, and speech therapists who wish to refer a patient.
Dr. Daniil Klimovich is trained in the management of temporomandibular disorders (TMD), orofacial pain, sleep apnea, and functional orthodontics. He is affiliated with the SSO, EOS, SEDCYDO, and EAOPD societies. The clinic offers:
- A complete assessment with appropriate imaging
- Multidisciplinary management combining physiotherapy, maxillofacial surgery, and sleep medicine
- Integrated management of TMJ and sleep disorders when both coexist
- A systematic report sent to the referring practitioner
To refer a patient or discuss a case, contact the clinic at 022 732 50 00 or via the contact form.
Frequently asked questions
Can TMJ disorders be cured?
In the majority of cases, yes. Most disorders progress favorably with conservative treatments such as splints and physiotherapy. Some chronic forms require longer follow-up, but they remain manageable.
How long does the treatment last?
It depends on the disorder. Muscle discomfort can improve in a few weeks, while disc displacement or osteoarthritis requires several months of follow-up. The treatment plan is defined after the diagnosis.
Is an MRI necessary?
Not always. MRI is useful for visualizing the disc and soft tissues in certain situations, but many cases are diagnosed through clinical examination and an X-ray. We prescribe imaging only when it changes the management approach.
Can TMJ and sleep apnea be treated at the same time?
In some cases, yes. When a TMJ disorder coexists with snoring or apnea, coordinated management can sometimes address both. This decision is based on a prior assessment.
Is a prescription needed to consult?
No. You can book an appointment directly, without going through another practitioner.
Book an appointment
Persistent jaw pain or locking does not always resolve on its own. An examination helps identify the cause and prevents it from becoming permanent.
Book an appointment with Dr. Daniil Klimovich for a complete evaluation of your TMJ and a tailored treatment plan.
DentalGeneva
Boulevard James-Fazy 4, 1201 Geneva
022 732 50 00
info@dentalgeneva.ch