

Dental pain is never a coincidence: it is often the sign of a biological or mechanical imbalance that must be identified quickly. In Geneva, the DentalGeneva clinic sees patients every week who ask themselves “where is this pain coming from?” Here are the most common causes, as well as those that are often overlooked, and finally clinical recommendations so that you know when to consult a professional.
Table of Contents
- Dental caries: more than just a cavity
- Pulp infection and periapical abscess: persistent pain
- Periodontal disease: when gums cause tooth pain
- Bruxism: the invisible grinding
- Tooth fracture or crack: “cracked tooth syndrome”
- Dentin hypersensitivity: understanding the hydrodynamic theory
- Non-odontogenic pain: when the culprit is hidden elsewhere
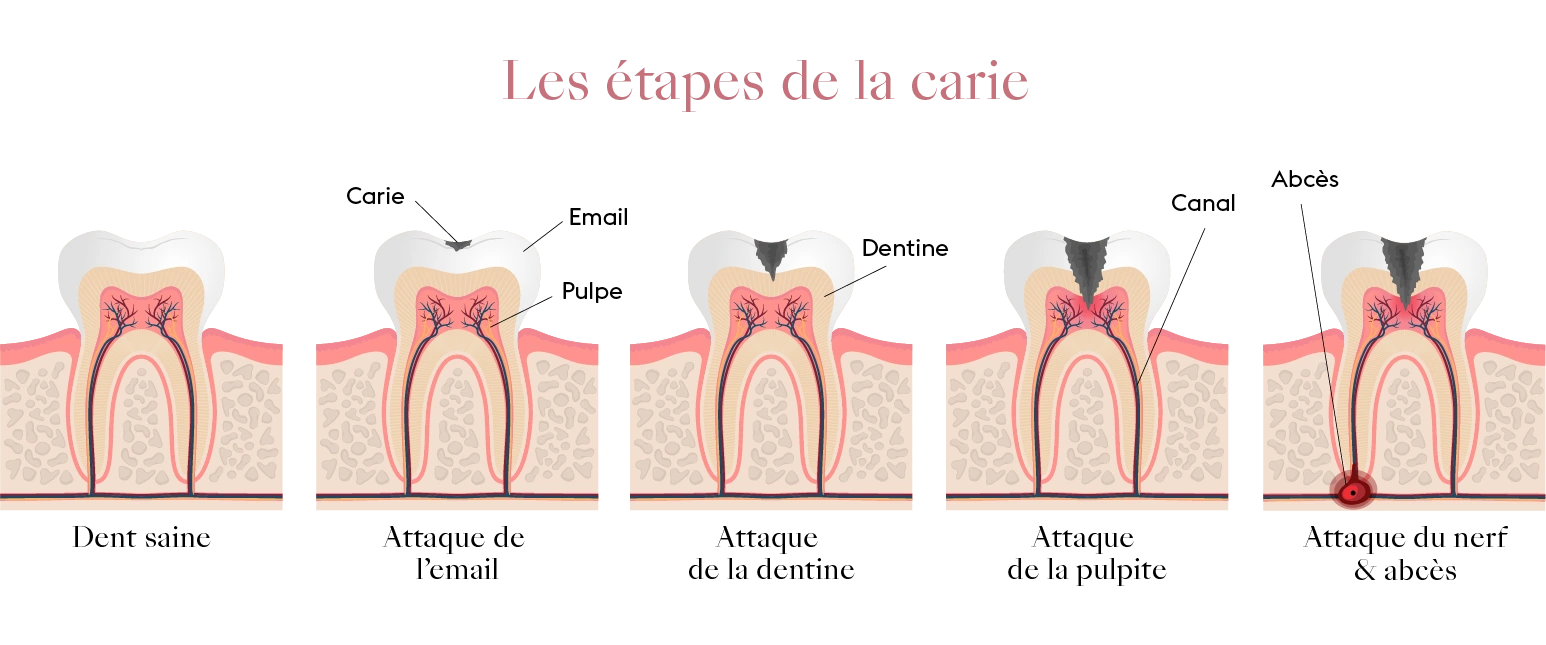
Dental caries: more than just a cavity
Oral bacteria transform sugars into acids that demineralize the enamel. If left untreated, the lesion reaches the dentin and then the pulp, causing very painful pulpitis. Today, cavities affect approximately 2 billion people worldwide and remain the most widespread non-communicable disease.
Key takeaway: pain often appears late; a semi-annual check-up allows for early, less invasive, and significantly less costly management.
Pulp infection and periapical abscess: persistent pain
As the cavity progresses, bacteria colonize the pulp and the infection reaches the apex; a periapical abscess forms, making chewing intolerable. This situation significantly increases dental anxiety and the consumption of analgesics. Acute cases require endodontic treatment or extraction.
Periodontal disease: when gums cause tooth pain
Periodontitis is a chronic infection of the supporting tissues of the tooth, notably the periodontal ligament and the alveolar bone. Untreated, it leads to progressive bone resorption, gingival recession, and then tooth mobility, often accompanied by localized pain, especially during mastication.
Periodontal pockets formed around the teeth become reservoirs for bacteria, sources of chronic inflammation and bad breath. In its aggressive or chronic forms, management relies on rigorous oral hygiene: twice-daily brushing with an appropriate technique, daily use of interdental brushes or floss, and, if necessary, a water flosser.
Recommended treatment protocols include mechanical debridement of the pockets (scaling and root planing), antimicrobial irrigation (chlorhexidine, hydrogen peroxide), and in certain cases, targeted antibiotic treatment or periodontal surgery.
Early screening by a dentist helps prevent advanced stages, which are often irreversible. DentalGeneva performs a complete periodontal assessment during every initial appointment.
Bruxism: the invisible grinding
Grinding or clenching teeth (often at night) progressively wears down the enamel, brings the dentin closer to nerve endings, and triggers permanent hypersensitivity. A multidisciplinary approach is recommended (stress management, occlusal splint, reduction of caffeine and nicotine).

Dr. Mariela Hernández Herrera
General Dentist. Dental Geneva, central Geneva.
Tooth fracture or crack: “cracked tooth syndrome”
An impact, a large filling, or chewing on hard food can cause a crack, often invisible to the naked eye. The tooth reacts with a brief but sharp pain upon release of pressure or exposure to cold. Diagnosis relies on transillumination and the temporary placement of a crown to immobilize the tooth.

Dentin hypersensitivity: understanding the hydrodynamic theory
In some patients, a simple draft of air triggers an electric pain: this is dentin hypersensitivity. Acid erosion, abrasive brushing, or frequent whitening expose the dentinal tubules. Brännström’s hydrodynamic theory explains that fluid movements stimulate pulp nociceptors.
What to do? Desensitizing toothpastes based on potassium nitrate, high-concentration fluoride varnish, glass ionomers, or resins if there is loss of substance.
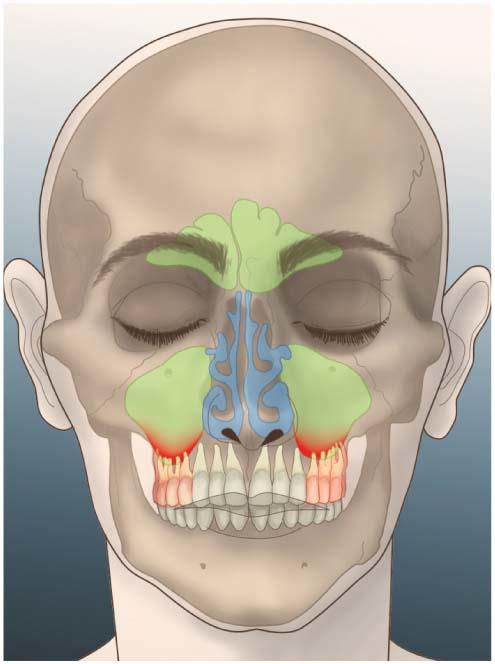
Non-odontogenic pain: when the culprit is hidden elsewhere
Maxillary sinusitis
The roots of the upper molars are in close contact with the sinus floor. A sinus infection, or conversely, a dental infection that reaches the sinus, causes diffuse pain, increased when leaning forward. The Swiss Medical Weekly estimates that approximately 10% of maxillary sinusitis cases are of dental origin.
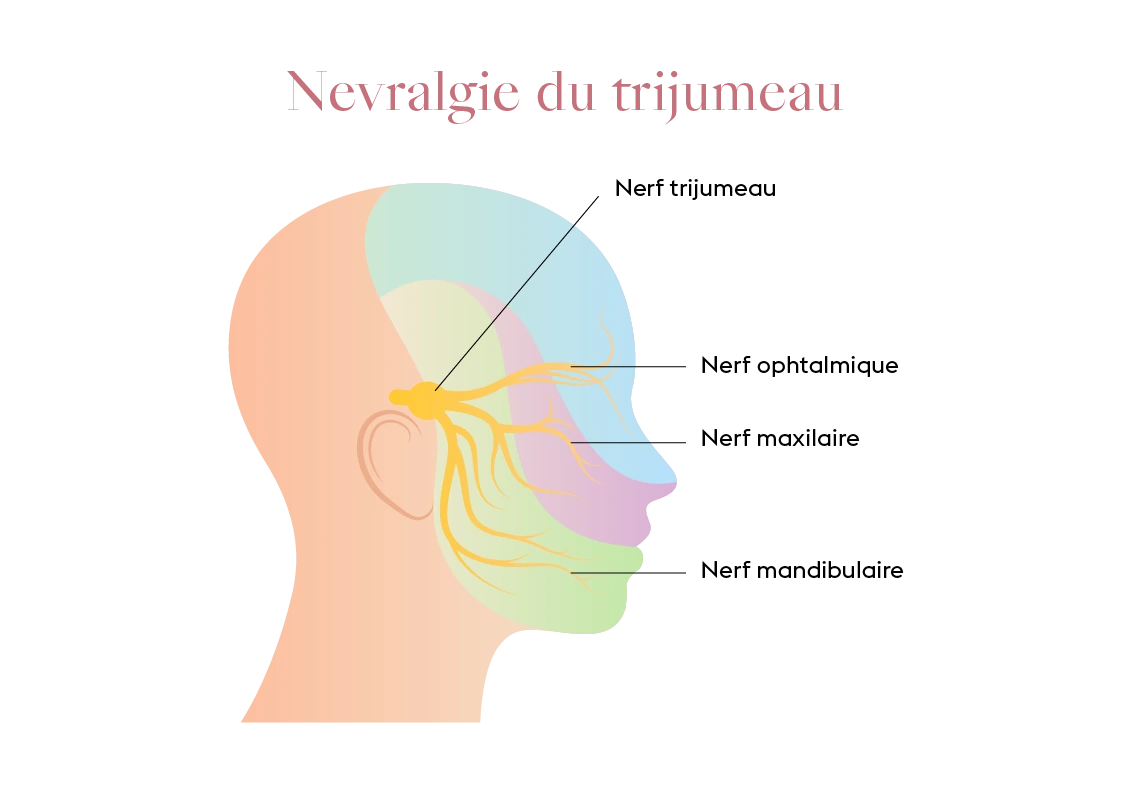
Trigeminal neuralgia
This neurological condition manifests as lightning-like electric shocks, sometimes interpreted as a toothache. In this case, dental treatment proves useless and often delays the diagnosis; a neuro-imaging assessment and the prescription of carbamazepine provide rapid relief.
When to consult DentalGeneva?
Pain that lasts more than 48 hours, wakes you up at night, or is accompanied by fever should lead you to make an appointment without delay. Our team, equipped with radiography, quickly identifies the cause and proposes the most conservative treatment possible.
Take care of your smile, as it is a lifelong health asset!